


Who Determines Long Term Health, the Mother or the Egg?
By Patricia Patnode

In the essay below, Dr. Darcy Bryan points out that an increasing number of studies are connecting maternal obesity to childhood obesity. Childhood obesity in turn significantly increases the likelihood of developing various health issues and complications (in childhood and as an adult) such as: Type 2 Diabetes, Cardiovascular Problems, Respiratory Issues, Fatty Liver Disease, Gastrointestinal Disorders, Early Onset of Puberty, amongst other issues.

It's important to recognize that childhood obesity is a complex issue influenced by genetics, lifestyle, and environmental factors. The recognition of such complications does not mean that there isn’t a responsibility for federal nutrition programs that feed children to structure themselves in order to imrpove health outcomes.
If the American taxpayer is footing the bill for a food-aid program, then the program should at least be structured to improve national health and not cause future health complications and, ultimately, Medicaid spending.
Highlights:
“Obesity in our mothers leads to obesity in our parents-to-be. Excessive weight gain during the first year of life and obesity in the preschool years increase lifetime risk of obesity in adulthood. This study further illustrates the importance of preventive health prior to conception. Pre-pregnancy obesity is significantly linked to early childhood obesity. Early childhood obesity results in a shorter, less healthy life..”
“A 2018 USDA study found that SNAP participation resulted in poorer nutritional status overall of the household. A recent review by Jerold Mande and Grace Flaherty found that children participating in SNAP were more likely to consume more sugar‐ sweetened beverages (SSBs), more high‐ fat dairy, and more processed meats than income‐ eligible nonparticipants, resulting in more lifetime risk of disease..”
“If the government is going to spend money mitigating nutritional shortcomings and poverty, then those programs should be structured in the most effective way possible to produce a healthier nation.”
Recommendations:
To bolster consumer demand for fresh fruits and vegetables, modify the Supplemental Nutrition Assistance Program (SNAP), which is the largest federal nutrition aid program and restrict clearly non-nutritious foods from SNAP eligibility.
The average American's caloric intake cannot be changed through regulation, but it can certainly be influenced through thoughtful nutrition education. Federal nutrition programs should improve nutritional education requirements, either through community centers, federal offices or via doctors visits.
The USDA’s guidelines for school lunch programs— programs that feed millions of children each day— must change to prioritize whole fruits, vegetables, healthy fats and meats, and allow for schools to tailor their menu to their community culture
Nutritional Support before Pregnancy is Critical – and Innovation Can Help
By Darcy Nikol Bryan, MD
As a practicing obstetrician for the past twenty years, I have seen the health of women change for the worse in the United States. The majority of patients I see now are at high risk during their pregnancies, due to diabetes, hypertension, or often both.
Most of the other experienced obstetricians I speak with feel the same. Deliveries have gotten harder and riskier.
The United States is falling behind in supporting the health of mothers and their babies. Maternal death rates have doubled over the past two decades from 9.8 per 100,000 live births in 2000 to 17.3 per 100,000 live births in 2018 [1]. There are multiple reasons for this increase in death from pregnancy, but probably the strongest is the obesity crisis [2]. Within my home state of Florida, a study evaluating pregnancy-related deaths from 1999 to 2012 found morbid obesity to be the most significant contributing factor to maternal death followed by late to no prenatal care [3]. Obesity in pregnancy is directly linked to the onset of gestational diabetes and hypertension along with risks of several life threatening conditions like pre-eclampsia [4]. Women are not the sole ones affected. Infant mortality increases linearly with rising maternal obesity [5].
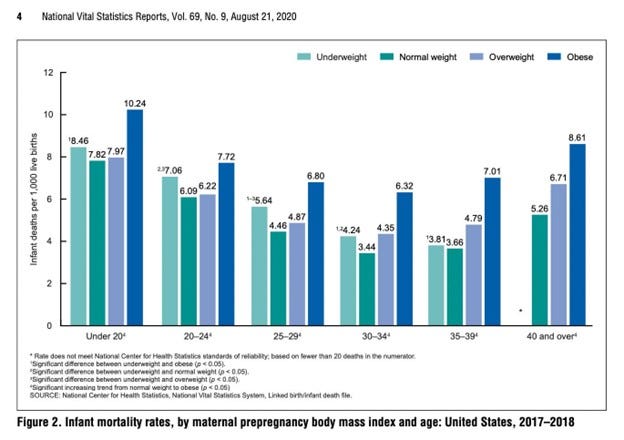
Source: https://www.cdc.gov/nchs/data/nvsr/nvsr69/NVSR-69-09-508.pdf
In 1974, the US Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) was established through the US Department of Agriculture to help low-income women and children under 5 years of age. WIC provides women and their young children supplemental foods, nutrition education, and breastfeeding support, all of which are immensely valuable for childhood development and maternal well-being [6].
Over the years of care, large WIC data sets have been collected which allow us to explore the impact of the obesity crisis. Analysis of a statewide Wisconsin WIC dataset evaluated 27,016 unique mother-child records between 2009 and 2011 [7]. The authors of the study saw a direct connection between preconception maternal weight and risk of childhood obesity. Children of mothers with excessive weight gain during pregnancy were 50% more likely to be obese, while the risk for childhood obesity increased by 4.5% for each 1kg/m2 increase in pre-pregnancy maternal BMI.
Obesity in mothers leads to obesity in parents-to-be. Excessive weight gain during the first year of life and obesity in the preschool years increase lifetime risk of obesity in adulthood [8]. This study further illustrates the importance of preventive health prior to conception. Pre-pregnancy obesity is significantly linked to early childhood obesity. Early childhood obesity results in a shorter, less healthy life [9].
At the time of WIC’s creation, the major concern was nutritional adequacy, not obesity [10]. Unlike the Supplemental Nutrition Assistance Program (SNAP), WIC provides participants with specific foods chosen by nutrition experts [11]. A recent systematic review of WIC related studies showed that participation in WIC was associated with improved birth outcomes and lower infant mortality [12]. As an example of the popularity of the program, women enrolled in WIC in the state of Illinois were interviewed and gave high value to the nutritional education received and WIC’s focus on supplying healthy foods [13]. In order to receive WIC funding, participating women are required to be educated on the importance of good nutrition, breastfeeding, risks of substance abuse, importance of childhood immunizations, and the value of folic acid before pregnancy [14].
WIC is the only nutrition assistance program with legislative and regulatory requirements to provide nutrition education to participants. Federal regulations require that WIC nutrition education be a benefit that is available at no cost to participants, be easily understood and bear a practical relationship to their nutritional needs, household situation and cultural preferences [15].
Strong evidence indicates that the status of a woman’s nutrition prior to pregnancy directly affects fetal gene expression at conception with resulting changes to a child’s long-term health [16]. This theory is known as the Developmental Origins of Health and Disease and was initiated by the Dutch Famine Studies (1944-1945) [17]. Data from that time showed that conception during acute starvation increased the rates of schizophrenia and cardiovascular disease in children born subsequently. Children of women who were further along in their pregnancies before the famine took place did not have similar long term health impacts. One can truly say that parenting begins before conception [18]. Basic science models have shown that a pre-implantation embryo is significantly altered by its nutritional environment [19]. Maternal nutritional factors are critical for the development of the placenta, whose general structure is formed within three weeks of conception.
Women know they have a problem with their health and want help. They want healthy babies, as evidenced by the interest in nutritional education from WIC recipients. A WIC clinic in Georgia conducted a trial providing preconception counseling while participants waited to be seen for their routine visits. A large majority of participants found the preconception counseling useful and important [20]. Women’s access to WIC only begins with pregnancy and during postpartum, missing the vital opportunity of preconception support. Healthy women tend to produce healthy babies. Both the Institute of Medicine and the American College of Obstetricians and Gynecologists have identified the preconception period as critical for minimizing adverse maternal and infant outcomes [21]. Government program support for preconception care is limited to non-existent. Benefits are available after pregnancy is diagnosed, downstream from the problem [22]. Malnutrition in the United States now presents itself as obesity from high caloric low nutrient foods, with low-income minority women particularly at risk [23].
So, the question becomes - how do we help low-income, reproductive-aged women planning for pregnancy obtain the nutritional education and support that reduces their risk for maternal mortality and other nutrition-related diseases?
One technological solution is pregnancy health applications. Lifestyle interventions can be effective in the management of obesity but need to be individualized, flexible, and culturally sensitive to be effective [24]. Patient self-management is also essential for decreasing the risk of developing chronic complications from obesity and requires immediate feedback with individualized treatment [25]. Mobile lifestyle apps geared towards pregnant women have increased in popularity and have the potential to positively support women in managing their nutritional needs [26].
Smartphones are widely used in the US and development of high-quality nutritional applications providing easy to understand advice holds promise. Compared with standard methods, artificial intelligence (AI) apps offer significant advantages for nutritional education and intervention [27]. For example, AI management of diabetes has increased significantly in recent years [28]. Ultimately, the goal is to integrate AI seamlessly with smart devices used at home, such as smartphones, wearables, medical devices, and sensor technology to improve patient health [29].
Application of AI in obesity management empowers patients to care for themselves, provides immediate lifestyle and dietary guidance, and works with clinicians in gathering data and guiding clinical decision making [30]. Projected advantages of AI’s use in patient management are lower cost, high efficiency, portability, and patient-centered productivity [31].
Another innovative approach would be supporting virtual health guidance with nutritional telemedicine. Mandating in-person visits exacerbates underlying barriers to preconception and prenatal care for women with social stressors, such as limited access to reliable transportation, unstable social situations (i.e homelessness), living in rural communities, or inflexible work and childcare schedules [32]. Implementation of obstetric telehealth holds promise for improving access to care. Multiple studies have compared health outcomes between in-person visit and telemedicine care models with no significant difference in obstetrical outcomes noted [33]. WIC can participate in these changes by expanding access to their telehealth programs.
As a nation, we need to look upstream where the problem starts – before pregnancy occurs – if we are to have any real hope of preventing childhood obesity and shortened American lifespans. Supporting innovative healthcare solutions and not being afraid to discuss the maternal health risks of obesity are good first steps to improving public health.
Darcy Nikol Bryan is an obstetrician gynecologist with an active practice at Women's Care Florida in Tampa. She earned an MD from Yale University’s School of Medicine and a Master's in Public Administration from the University of Texas at Arlington. She is a certified remote pilot and student private pilot. Her research encompasses public policy and the impact of technology on healthcare provision. She co-authored the book Women Warriors: A History of Courage in the Battle Against Cancer.
Further Reading:
Part 2: Solutions For The Failing School Lunch System By Juliana Sweeny for Farming Abundance
Part 1: The Problem - School Lunches Are Failing Our Children By Juliana Sweeny for Farming Abundance
SNAP can improve nutrition, help farmers, and support the environment By Angela Rachidi for Farming Abundance
Nobody Is Poisoning Your Groceries By David Norcross and Patricia Patnode
Sources:
1. Centers for Disease Control and Prevention (n.d.) Pregnancy mortality surveillance system. Reproductive Health. Retrieved February 11, 2023, from https://www.cdc.gov/reproductivehealth/maternal-mortality/pregnancy-mortality-surveillance-system.htm
2. Redman, LM & Phelan, S. (2016). It is time to take preconception health seriously. Obesity (Silver Spring, Md.), 24(2), 279–279. https://doi.org/10.1002/oby.21375
3. Hernandez, L., Sappenfield, W. M., Harris, K., Burch, D., Hill, W. C., Clark, C. L., & Delke, I. (2018). Pregnancy-Related Deaths, Florida, 1999–2012: Opportunities to Improve Maternal Outcomes. Maternal and Child Health Journal, 22(2), 204–215. https://doi.org/10.1007/s10995-017-2392-y
4. Hernandez, L., Sappenfield, W. M., Harris, K., Burch, D., Hill, W. C., Clark, C. L., & Delke, I. (2018). Pregnancy-Related Deaths, Florida, 1999–2012: Opportunities to Improve Maternal Outcomes. Maternal and Child Health Journal, 22(2), 204–215. https://doi.org/10.1007/s10995-017-2392-y
5. Bodnar, L., Siminerio, L. L., Himes, K. P., Hutcheon, J. A., Lash, T. L., Parisi, S. M., & Abrams, B. (2016). Maternal obesity and gestational weight gain are risk factors for infant death. Obesity (Silver Spring, Md.), 24(2), 490–498. https://doi.org/10.1002/oby.21335
6. https://www.fns.usda.gov/wic
7. Ohlendorf, JM, Robinson, K., & Garnier-Villarreal, M. (2019). The impact of maternal BMI, gestational weight gain, and breastfeeding on early childhood weight: Analysis of a statewide WIC dataset. Preventive Medicine, 118, 210–215. https://doi.org/10.1016/j.ypmed.2018.11.001
8. Andrea, SB, Hooker, E. R., Messer, L. C., Tandy, T., & Boone-Heinonen, J. (2017). Does the association between early life growth and later obesity differ by race/ethnicity or socioeconomic status? A systematic review. Annals of Epidemiology, 27(9), 583–592.e5. https://doi.org/10.1016/j.annepidem.2017.08.019
9. Lindberg L, Danielsson P, Persson M, Marcus C, Hagman E. (2020). Association of childhood obesity with risk of early all-cause and cause-specific mortality: A Swedish prospective cohort study. PLoS Med, 17(3):e1003078. doi: 10.1371/journal.pmed.1003078.
10. Kennedy, E. & Guthrie, J. F. (2016). Nutrition Assistance Programs: Cause or Solution to Obesity. Current Obesity Reports, 5(2), 176–183. https://doi.org/10.1007/s13679-016-0207-x
11. Kennedy, E. & Guthrie, J. F. (2016). Nutrition Assistance Programs: Cause or Solution to Obesity. Current Obesity Reports, 5(2), 176–183. https://doi.org/10.1007/s13679-016-0207-x
12. Venkataramani, M., Ogunwole, S. M., Caulfield, L. E., Sharma, R., Zhang, A., Gross, S. M., Hurley, K. M., Lerman, J. L., Bass, E. B., & Bennett, W. L. (2022). Maternal, Infant, and Child Health Outcomes Associated With the Special Supplemental Nutrition Program for Women, Infants, and Children: A Systematic Review. Annals of Internal Medicine, 175(10), 1411–1422. https://doi.org/10.7326/M22-0604
13. Weber, SJ., Wichelecki, J., Chavez, N., Bess, S., Reese, L., & Odoms-Young, A. (2019). Understanding the factors influencing low-income caregivers’ perceived value of a federal nutrition programme, the Special Supplemental Nutrition Program for Women, Infants and Children (WIC). Public Health Nutrition, 22(6), 1056–1065. https://doi.org/10.1017/S1368980018003336
14. https://www.ncdhhs.gov/chapter5102021pdf/download?attachment
15. Specified in sections 17(b)(7), 17(f)(1)(C)(x), and 17(j) of the Child Nutrition Act of 1966, as amended, and the Federal WIC regulations in sections 246.2 and 246.11.
16. King, J. (2016). A Summary of Pathways or Mechanisms Linking Preconception Maternal Nutrition with Birth Outcomes. The Journal of Nutrition, 146(7), 1437S–1444S. https://doi.org/10.3945/jn.115.223479
17. Stein, Z. & Susser, M. (1975). The Dutch famine, 1944-1945, and the reproductive process. II. Interrelations of caloric rations and six indices at birth. Pediatric Research, 9(2), 76–83. https://doi.org/10.1203/00006450-197502000-00004
18. Lane, M., Robker, R. L., & Robertson, S. A. (2014). Parenting from before conception. Science (American Association for the Advancement of Science), 345(6198), 756–760. https://doi.org/10.1126/science.1254400
19. New Findings on Dietary Proteins Described by Investigators at Aston University (Do little embryos make big decisions? How maternal dietary protein restriction can permanently change an embryo’s potential, affecting adult health) (p. 456–). (2015). NewsRX LLC
20. Dunlop, A., Dretler, A. W., Badal, H. J., & Logue, K. M. (2013). Acceptability and Potential Impact of Brief Preconception Health Risk Assessment and Counseling in the WIC Setting. American Journal of Health Promotion, 27(3_suppl), S58–S65. https://doi.org/10.4278/ajhp.120109-QUAL-7
21. Healthy People - Healthy People 2020 (cdc.gov)
22. Redman, LM & Phelan, S. (2016). It is time to take preconception health seriously. Obesity (Silver Spring, Md.), 24(2), 279–279. https://doi.org/10.1002/oby.21375
23. Gilmore, LA., Augustyn, M., Gross, S. M., Vallo, P. M., Paige, D. M., & Redman, L. M. (2019). Periconception weight management in the Women, Infants, and Children program. Obesity Science & Practice, 5(2), 95–102. https://doi.org/10.1002/osp4.327
24. Chen, Moran, L. J., Harrison, C. L., Ukke, G. G., Sood, S., Bennett, C. J., Bahri Khomami, M., Absetz, P., Teede, H., & Lim, S. (2022). Ethnic differences in response to lifestyle intervention for the prevention of type 2 diabetes in adults: A systematic review and meta‐analysis. Obesity Reviews, 23(1), e13340–n/a. https://doi.org/10.1111/obr.13340.
25. Funnell, Brown, T. L., Childs, B. P., Haas, L. B., Hosey, G. M., Jensen, B., Maryniuk, M., Peyrot, M., Piette, J. D., Reader, D., Siminerio, L. M., Weinger, K., & Weiss, M. A. (2012). National standards for diabetes self-management education. Diabetes Care, 35(1), S101–S108. https://doi.org/10.2337/dc12-s101.
26. Tripp, Hainey, K., Liu, A., Poulton, A., Peek, M., Kim, J., & Nanan, R. (2014). An emerging model of maternity care: Smartphone, midwife, doctor? Women and Birth : Journal of the Australian College of Midwives, 27(1), 64–67. https://doi.org/10.1016/j.wombi.2013.11.001.
27. Li, Huang, J., Zheng, L., & Li, X. (2020). Application of artificial intelligence in diabetes education and management: present status and promising prospect. Frontiers in Public Health, 8, 173–173. https://doi.org/10.3389/fpubh.2020.00173.
28. Makroum, M., Adda, M., Bouzouane, A., & Ibrahim, H. (2022). Machine learning and smart devices for diabetes management: systematic review. Sensors (Basel, Switzerland), 22(5), 1843–1867. https://doi.org/10.3390/s22051843
29. Ibid.
30. Peleg, M, Shahar, Y., Quaglini, S., Broens, T., Budasu, R., Fung, N., Fux, A., García-Sáez, G., Goldstein, A., González-Ferrer, A., Hermens, H., Hernando, M. E., Jones, V., Klebanov, G., Klimov, D., Knoppel, D., Larburu, N., Marcos, C., Martínez-Sarriegui, I., … van Schooten, B. (2017). Assessment of a personalized and distributed patient guidance system. International Journal of Medical Informatics (Shannon, Ireland), 101, 108–130. https://doi.org/10.1016/j.ijmedinf.2017.02.010.
31. Li, Huang, J., Zheng, L., & Li, X. (2020). Application of artificial intelligence in diabetes education and management: present status and promising prospect. Frontiers in Public Health, 8, 173–173. https://doi.org/10.3389/fpubh.2020.00173.
32. Fryer, K., Delgado, A., Foti, T., Reid, C. N., & Marshall, J. (2020). Implementation of Obstetric Telehealth During COVID-19 and Beyond. Maternal and Child Health Journal, 24(9), 1104–1110. https://doi.org/10.1007/s10995-020-02967-7.
33. Wu, K., Lopez, C., & Nichols, M. (2022). Virtual Visits in Prenatal Care: An Integrative Review. Journal of Midwifery & Women’s Health, 67(1), 39–52. https://doi.org/10.1111/jmwh.13284.